As we look to the future, it is well within our grasp that Australia will be the first country to eliminate cervical cancer.
As we look to the future, it is well within our grasp that Australia will be the first country to eliminate cervical cancer. Australia is a global leader in cervical cancer prevention – offering routine Cervical Screening Tests to women aged 25 – 74 years of age and vaccination against Human Papillomavirus (HPV), which is responsible for virtually all cases of cervical cancer, delivered to adolescents in their first year of secondary school.
Some may say our work here is done, but under the glitter of success the uncomfortable truth persists. The inequitable burden of cervical cancer among Aboriginal and Torres Strait Islander women is profound – deafening – and yet silenced in every way possible.
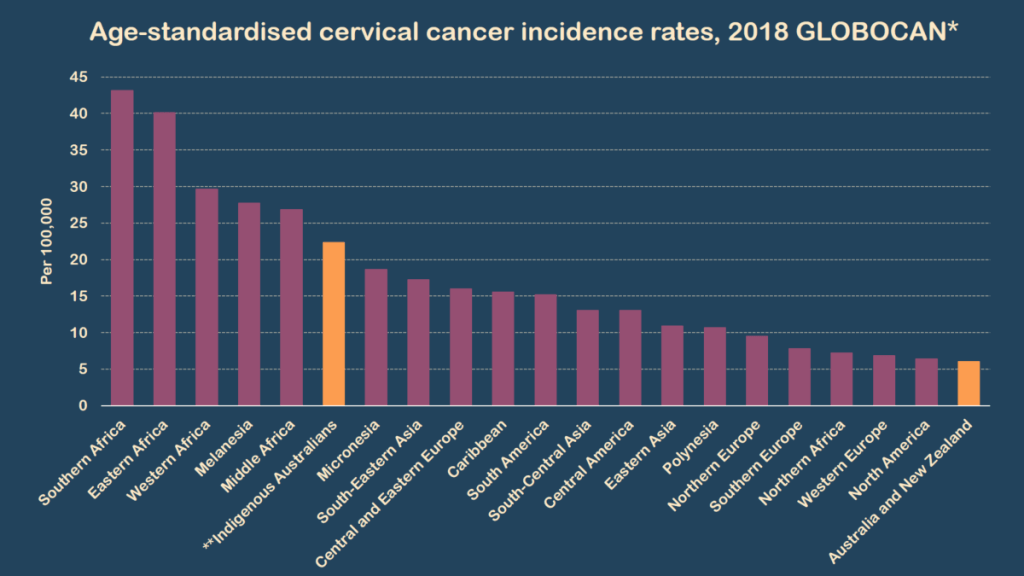
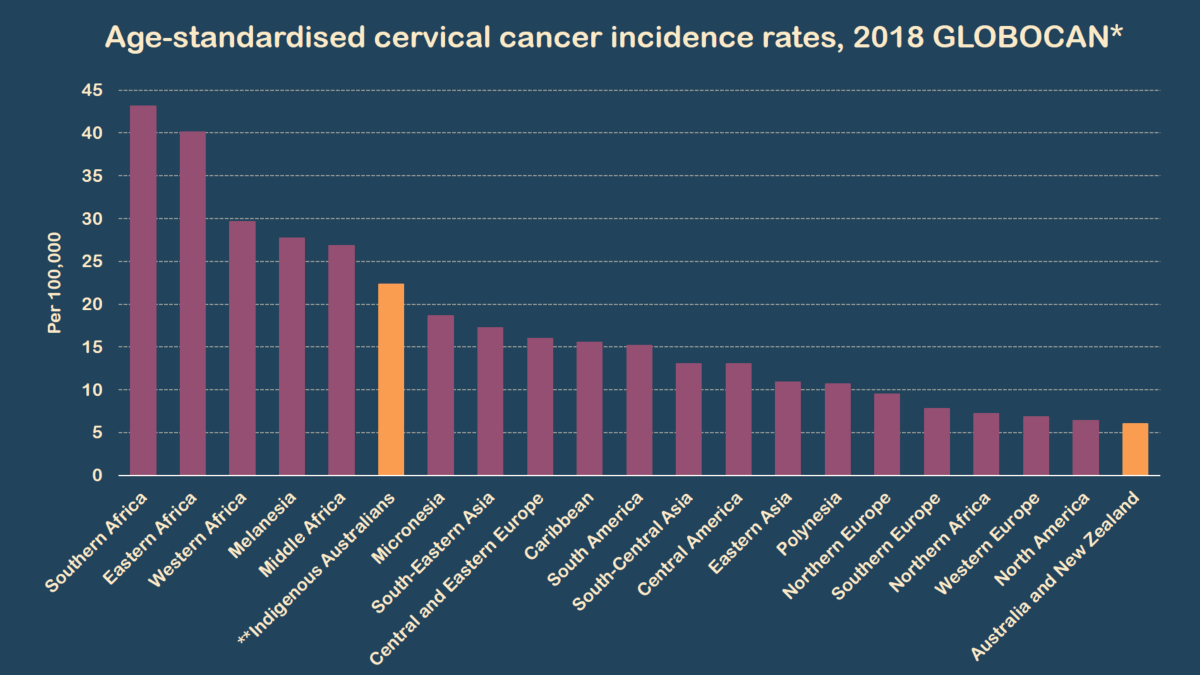
The inequity is obvious and supported by strong epidemiological evidence. Aboriginal and Torres Strait Islander women are twice as likely to be diagnosed with cervical cancer and over three times as likely to die from cervical cancer than other Australian women. In fact, while non-Indigenous Australian women experience one of the lowest cervical cancer incidence rates in the world Aboriginal and Torres Strait Islander women experience incidence rates similar to women living in less developed regions.
*Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 12 June 2019. **Australian Institute of Health and Welfare 2019. Cervical screening in Australia 2019. Cancer series no. 123. Cat. no. CAN 124. Canberra: AIHW.
Our work in Queensland demonstrates that the majority of Aboriginal and Torres Strait Islander women do not participate in cervical screening, but for those that do they become regular screeners. We also were able to demonstrate that Aboriginal and Torres Strait Islander women were least likely to screen in the age-group they were most likely to be diagnosed with cervical cancer. This was the first-time population based estimates were able to be produced for Aboriginal and Torres Strait Islander women 25 years after the National Cervical Screening Program was implemented.
In 2018 my team hit the road to yarn with Aboriginal and Torres Strait Islander women who participate or never/rarely participate in cervical screening to understand their experiences and perspectives. We talked with 80 Aboriginal and Torres Strait Islander women – 50 who had participated in screening in the past five years and 30 who had not. We went to five sites across New South Wales, Queensland and Northern Territory with a mixture of government run primary health care services with a large number of Aboriginal and Torres Strait Islander clients, and Aboriginal Community Controlled Health Services.
Our approach to this research was to centre the voices of Aboriginal and Torres Strait Islander women in every aspect of the research. All interviewers were Aboriginal and Torres Strait Islander women, and this provided a platform in which Aboriginal and Torres Strait Islander women could share their experiences with a criticality that I that may not possible with non-Indigenous researchers. The engagement with health services were also enhanced as we connected with other Aboriginal and Torres Strait Islander staff at the health centres. These staff were critical to the success of how we were received in the community and the way in which we recruited participants, and their labour does not go unrecognised.
We are yet to finalise our results but in recognising the sovereignty of Aboriginal and Torres Strait Islander women, it was clear to me that control over decision-making and trust are a fundamental part of cervical screening stories. Almost all of the Aboriginal and Torres Strait Islander women who never or rarely screened reflected that this was the first time anyone had ever asked them “why?”.
I also recognised that health services or health practitioners do not have an immediate position of safety for Aboriginal and Torres Strait Islander women. This was evident in two ways – for some women who had a trusting relationship with their doctor they were willing to forgo preventative health services in order to keep that relationship, while for others the trauma they had experienced within a health setting imposed a major obstacle to cervical screening. As we analyse the results we are reflecting on the foundational work of others including the late Maureen Kirk, an Aboriginal woman who pioneered this space. I am building on the labour of my long-term mentor Professor Gail Garvey who has fought for cancer to be on the agenda for Aboriginal and Torres Strait Islander people while building a research agenda and workforce to support it.
Despite the unacceptable inequity illustrated by the statistics, they have been unable to galvanise action. The stories provide the contextual understanding of ‘why’ and the authority in which they are told saw me move from the knower to the learner. As an epidemiologist I had to trade in the numbers and my positivist position – of neutrality and objectivity. I know the power of story-telling as a Torres Strait Islander woman and the power it has played and continues to play in our survival. The data from the stories are a critical addition to the epidemiological data.
I hear the collective groan when I remind Governments and Researchers that Australia is not the success story they like to tell and have beared the brunt of the colonial mechanisms they have used to try and silence me. My role in the academy is one of activism, built on and made possible because of the leadership of the Black Women before me and those who shared their stories.
And so in their legacy, I will continue the fight.
Authors note: the statements made in this article reflect those of the author and results from the Screening Matters study are forthcoming.
A reflection on Sorry Day and Reconciliation Week 2026
It’s Sorry Day and Reconciliation week and I’m reminded again that language matters. White people tell me this constantly. Use the right language. Tone it…
The ACT appoints its first Aboriginal Chief Coroner, After Years of Calling For Justice for Aboriginal Deaths in Custody
This article includes the names of Aboriginal People who have died, and mentions instances of racism. History has been made with the announcement of the…
Subscribe
I would like to receive the IndigenousX monthly newsletter
 *Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 12 June 2019. **Australian Institute of Health and Welfare 2019. Cervical screening in Australia 2019. Cancer series no. 123. Cat. no. CAN 124. Canberra: AIHW.
*Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 12 June 2019. **Australian Institute of Health and Welfare 2019. Cervical screening in Australia 2019. Cancer series no. 123. Cat. no. CAN 124. Canberra: AIHW.

 *Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 12 June 2019. **Australian Institute of Health and Welfare 2019. Cervical screening in Australia 2019. Cancer series no. 123. Cat. no. CAN 124. Canberra: AIHW.
*Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 12 June 2019. **Australian Institute of Health and Welfare 2019. Cervical screening in Australia 2019. Cancer series no. 123. Cat. no. CAN 124. Canberra: AIHW.
